Dietitian Blog | May 9 2023
Anemia in the elderly: Normal aging or cause for concern?

Anemia develops when the blood produces a reduced amount of healthy red blood cells. This reduction impacts the body’s ability to transport oxygen to all tissues and impacts functional ability and quality of life. It is estimated that 15% of seniors aged 60+ are anemic. Is this a normal part of aging or a clinical condition requiring further investigation? Due to anemia’s significant impact on functional ability and quality of life, all patients with this condition should be evaluated to ensure proper treatment is provided.
Scope of the problem
It’s estimated that 15% of seniors aged 60+ are anemic. Recent studies on this patient population have shown a higher risk of poor health outcomes, diminished functional capacity, cognitive decline, poor quality of life, depression, sarcopenia, and low muscle quality. With the elderly making up 52 million of the US population as of 2018, this is an alarming concern.
Functional assessments have demonstrated differences between patients with and without anemia. A lower hemoglobin value has been associated with low aerobic capacity, strength, and endurance. A slower walking speed is a powerful predictor of disability, need for institutional care, and death. Furthermore, anemia has been associated with increased rates of cardiac death and major adverse clinical events.
In the United States, anemia is four times more prevalent in nursing home residents than the community dwelling population. A higher prevalence is also noted in both men and women of African American ethnicity. In fact, African American women aged 80 to 85 years have been shown to be six times more likely to be anemic compared to the general population.
Economic cost
Anemia results in 2.8 million physician office visits and 890,000 emergency department visits per year.
Twenty-five percent of patients admitted to the hospital for anemia are readmitted within 30 days. When admitted, anemia is associated with elevated hospital mortality and longer length of stay. Adjusted length of stay is estimated to be four to five days longer with moderate anemia and seven to ten days longer with severe anemia.
The etiology of anemia
The causes of anemia can be separated into several groups:
- Deficiency of nutrients – including iron (most common), vitamin B12, folic acid, copper, and zinc
- Anemia of inflammation or chronic disease – such as congestive heart failure (CHF), malignancy, auto-immune disease, and infection
- Chronic kidney disease (CKD)
- Hematologic malignancies
- Unexplained anemia of aging
The third National Health and Nutrition Examination Survey (NHANES) identified 1 in 3 cases of anemia could be attributed to nutritional causes, and another 1 in 3 was associated with inflammation or CKD. The rest were determined to be due to unexplained anemia of aging, which is a diagnosis of exclusion. Chronic anemia is a gradual decline in red blood cells, and its symptoms include headaches, weakness, vertigo, faintness, and pale skin.
Relevant laboratory values
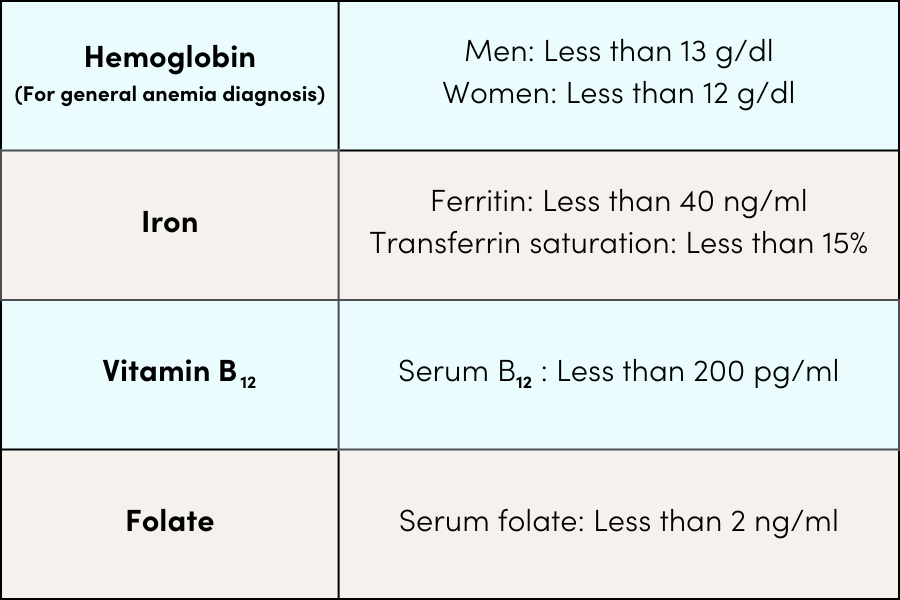
The World Health Organization defines anemia as hemoglobin concentration less than 12 g/dl in women and less than 13 g/dl in men. Serum ferritin is the best indicator to define iron deficiency. However, ferritin is an acute phase reactant and can be falsely high in setting of infection and/or inflammation.
Lab parameters for anemia
Treatment
Treatment of anemia in the elderly depends largely on the underlying cause. Diet enrichment and alcohol abstinence are vital for correcting nutritional deficiencies. Oral supplements continue to play a major role and are a simple first step in replacement.
Ferrous sulfate contains the highest amount of elemental iron, but can also be the most poorly tolerated. Better tolerance to ferrous gluconate and ferrous fumarate has been demonstrated. The dosage of these alternatives needs to be adjusted to make up for the lower level of elemental iron. While the patient may feel better within several days after starting treatment, it may take several months to resolve the deficiency.
Symptomatic patients with serum hemoglobin less than 8 g/dl may require intravenous iron therapy. Medications such as erythropoietin stimulating agents are used in CKD.
Vitamin B12 deficiency can occur from an inadequate diet but is more often associated with other conditions, including:
- Lack of intrinsic factor
- Alcohol consumption
- Medication such as proton pump inhibitors, antacids, metformin ]Medical conditions such as, thyroid disease, celiac disease, H. pylori infection, Crohn’s disease
- Gastrointestinal surgeries
Folate deficiency has become less common with the fortification of
grain products with B vitamins. Food sources of folate include leafy green vegetables, citrus fruits, beans, and whole grains. Treatment of the deficiency includes a well-balanced diet, folic acid supplements, and treating the underlying cause.
Prevention
Ultimately, addressing the physiological cause of anemia is the first step in prevention. Consuming foods rich in iron and vitamin C can help halt the progression of anemia. The foods below should be incorporated into the average daily diet for geriatric patients due to their elevated risk of this condition.
Good sources of iron include:
- Beans
- Dried fruit
- Eggs
- Lean red meat
- Salmon
- Iron-fortified breads and cereals
- Chickpeas
- Tofu
- Dark green leafy vegetables
Vitamin C sources include: (help absorb iron)
- Oranges
- Grapefruits
- Strawberries
- Tomatoes
- Kiwis
Dietitians On Demand is a nationwide staffing and recruiting company for registered dietitians, specializing in short-term, temporary and permanent-hire positions in acute care, long term care and food service positions. We’re dedicated to dietitians and helping them enhance their practice and excel in the workplace. Check out our job openings, request your coverage, or visit our store today!
References:
Clinical and hematological evaluation of geriatric anemia. S. Krishnamurthy,et al. Journal of Family Medicine and Primary Care. 2022; 11:3028-33.
Unexplained anemia of aging: Etiology,health consequences, and diagnostic criteria. J Guralnik, et al. Journal of the American Geriatrics Society. 2022:70:891-899.
Does Aging have an impact on hemoglobin? Study in elderly population at rural teaching hospital. N Raisinghani,et al. J Family Med Prim Care 2019;8:3345-9.
Anemia in Elderly Persons. K Olmedo. Oct 4, 2022https://emedicine.medscape.com/article/1339998
Individualized treatment for iron deficiency anemia in adults. M Alleyne, et al. Am J Med 2008 Nov; 121(11):943-948.
Population Reference Bureau. prb.org/resources/fact-sheet-aging-in-the-United-States/ July 15, 2019.

About Patricia Nicholas
Patricia Nicholas, MS, RD, CSG, CDN is passionate about improving life for seniors in the community, inpatient, home care and long-term care settings. She stresses healthy food over medications. Along with her patient care experience, she has a background in classroom instruction and clinical and food service management.
Who we are
Dietitians On Demand is the nationwide leader in providing dietitians with jobs they love. If flexibility, competitive pay, a full benefits package, free CPEUs each month and a team dedicated to dietitians sound good to you, apply to our positions today.


